

“Regulate the breathing, and thereby control the mind.” — B.K.S. Iyengar (1918-2014)
What is breathing? Breathing is the exchange of gasses used by land animals to provide their bodies’ cells with the oxygen. They need that oxygen to burn food into energy. Oxygen allows cells to break down sugars derived from food and provide us with energy to move and think. Breathing takes many forms. For example, crickets simply circulate air through open tubes while fish use gills to collect oxygen from water.
In animals with lungs, breathing is called “ventilation.” During the ventilatory process, air is pulled into the lungs, where gas exchange takes place. Oxygen diffuses from the air into the blood during inhalation, and carbon dioxide diffuses from the blood into the air during exhalation. When the environment requires that an animal move more than usual, its breathing rate increases so that more oxygen can be delivered to its busy cells.

Illustration 3.1: A. Circulatory system of a cricket; B. Gills of a salmon
Mammals have muscles in the chest that act to inflate and deflate the lungs. The most important of these is a specialized muscle located beneath the lungs called the respiratory diaphragm. Other land vertebrates, including amphibians, reptiles, and the late dinosaurs exhibit a similar structure, although theirs is simpler and sits above the lungs rather than below. The mammalian diaphragm changes its behavior depending on the immediate circumstances, focusing on efficiency in safe environments but producing paranoid overexertion in threatening ones. This chapter will describe how stress causes the diaphragm to produce quick, shallow strokes, and how deliberately practicing longer, fuller breaths can reinstate its proper function.
Distressed Breathing vs. Diaphragmatic Breathing
Breathing shallowly, at short intervals, is known as distressed breathing. It is also known as defensive breathing, nondiaphragmatic breathing, or thoracic breathing. The behavior is strongly associated with stress and anxiety disorders and tends to cause nervousness and discomfort. Distressed breathing is characterized by rapid, uneven breaths, punctuated by gasps, sighs, and breath holding. It can easily become habitual, leading to serious long-term dysfunction.1
Distressed breathing has a reciprocal relationship with the brain’s stress and threat response systems. We breathe more defensively when we are afraid, and we become more afraid when we breathe defensively. Distressed breathing is also used as a signal of submission. This is why improving your breathing will not only help you control negative thinking but also help you become more dominant. Indeed, you will find that true diaphragmatic breathing is incompatible with anxiety, social and otherwise.
People who breathe shallowly are usually unaware of the condition and do it unknowingly throughout the day. Most of us breathe by default with “bated breath.” We wait for everything in our lives with abated breathing as if a judge were about to announce our prison sentence. We do this even when circumstances are normal and unthreatening. Everyone understands more or less instinctively that inhibited, irregular breathing is a source of tension and stress. This is clear from the popularity of idioms like “waiting to exhale,” “sigh of relief,” “couldn’t catch my breath,” “breath of fresh air,” “give me some breathing room,” and “short of breath.”
Breathing patterns are contagious and often modeled. Children learn how to breathe from their parents. For this reason, children often take on the anxiety level of their parents. We perceive others’ breathing patterns from their movements, speech patterns, sounds of inhalation and exhalation, and facial tension. We all alter our breathing to accommodate, or match, that of the people around us. I saw this clearly when my distressed breathing would contaminate the breathing of others.
Is your breathing unhealthy? Likely so. Imagine that you are threading a small needle with a thin thread. As you line up the thread with the hole, are you holding your breath? You shouldn’t be. Experience pronounced distressed breathing firsthand by doing the following activity:

After performing this activity, most people report uncomfortable sensations such as anxiety, panic, or tension, accompanied by increased heart rate, physical agitation, breathlessness, chest pressure, or even the feeling of starving for air. These are the typical outcomes of distressed breathing, and many of us unnecessarily subject ourselves to them daily. An anxious person will breathe at an average rate of 18 to 20 breaths per minute. A relaxed person practicing diaphragmatic breathing will breathe only five to seven times per minute.2 Problems with diaphragmatic breathing are best conceptualized as falling on a continuum rather than as a threshold. There are no firm diagnostic criteria for distressed breathing; virtually everyone is somewhere on the spectrum.
Newborns breathe diaphragmatically, but, by age ten, diaphragmatic function is usually minimized. This is because few of us experience childhoods that our bodies interpret as optimal. The transition away from diaphragmatic breathing occurs during early childhood as we learn which environmental stimuli should be linked to concern and worry. The process is normal and prepares us to be especially cautious in specific situations. However, by the time we reach adulthood, nearly every situation recruits distressed breathing, just some more than others.3 Distressed breathing is implicitly conditioned to occur alongside many activities and postures, and these associations are often never unlearned. That leaves us gasping when the telephone rings, holding our breath while sitting at the keyboard, and hyperventilating during everyday conversations.
We cannot immediately switch from distressed breathing to competent, calm, diaphragmatic breathing because we are held back by long-term physiological changes wrought by years of breathing shallowly. These changes involve a multitude of alterations to the muscles and nerves of the respiratory system. They cause the diaphragm to atrophy and become stuck in partial contraction. These changes are driven by gene activity, constitute developmental plasticity, and are largely responsible for the sympathetic overactivation discussed in the last chapter. Fortunately, the changes are reversible. However, you cannot pay anybody to retrain your breathing for you, and there is no pill you can take. It requires time and discipline. As with the other exercises in this book, you will find the breathwork rewarding once you start to see the results.
Many therapists, books, and self-help resources promote breathing exercises. Most of these exercises last only a few seconds, are intended to counteract panic attacks, and come with no guidelines for permanently changing breathing style. Moreover, users are often only told to “breathe deeply” or “focus on the breath” without being provided any further instructions. Simply focusing on the breath is beneficial because it prompts the individual to note when their breath is unnaturally shallow. It causes the person to think, “Wait, my current predicament is not all that bad, so why am I breathing like there is something at stake?” That is a productive first step.
Awareness of desperation in the breath is a start, but it does not address the problem at its source. Rather than simply focusing on the breath, we need to actively lengthen and deepen our breaths throughout the day to strengthen the muscles and reprogram the unconscious breathing circuits in our brainstems. Consciously overriding its injurious commands will rewire your brain and retune your entire body.
Diaphragmatic Breathing Utilizes the Respiratory Diaphragm
Deep, non-distressed breathing is controlled by the diaphragm, a dome-shaped skeletal muscle that separates the thorax (containing the heart and lungs) from the abdomen (containing the intestines, stomach, liver, and kidneys). Only an eighth of an inch thick, it extends across the bottom of the rib cage and moves air into and out of the lungs by changing shape. It moves like a plunger. When it contracts, the diaphragm moves downward, drawing in breath, resulting in inhalation. When it relaxes, it moves upward, expelling air and causing you to exhale. The diaphragm can move as much as ten centimeters, but many adults use only around one centimeter or 10% of the total range. Expanding the range of your diaphragm is essential, and I designed this chapter’s exercises to do just that. But first, let’s explore how to move the diaphragm at all.
Diaphragmatic breathing, also known as eupnea in the scientific literature and belly breathing in the vernacular, is an unlabored form of breathing seen in untraumatized mammals. You should be able to observe it in any young mammal resting peacefully.4 It is easiest to spot in a sleeping infant, a kitten, or a puppy lying on its side. The animal’s stomach will move up and down with each breath. How do you know whether you are breathing with your diaphragm? Your belly should move in much the same way. Use the conventional guidelines for belly breathing in the activity below:

Illustration 3.2: A. Belly breather ensuring that the stomach rises and falls; B. Motion of the diaphragm during breathing.
The motion of one’s stomach is the telltale sign of diaphragmatic breathing, and this method works for many people.5 However, most instructions for diaphragmatic breathing end here. This was discouraging for me because I felt there should be a more substantial protocol. Moreover, I realized my stomach was rising and falling only because I was using my abdominal muscles, rather than my diaphragm, to suck it in and push it out. No matter how I tried to vary my approach to each breath, my stomach would not move unless I used my abdominals to move it. My diaphragm was so tense that monitoring the motion of my stomach did nothing for me. I wonder how many other people following these guidelines simply use their abdominal muscles to mimic the movement without breathing diaphragmatically.
After years of exhaustively reading the medical literature on anxiety, I became convinced that my problem lay with my dysfunctional breathing style. I was determined to correct it but couldn’t find anything that explained how. I would lay on the ground for hours trying to perceive the movement of my diaphragm to no avail. The diaphragm has relatively few proprioceptive nerve endings, meaning that it is difficult to tell how much it is contracting and where it is in space. That makes it very difficult to perceive consciously, which makes the problem all the worse.
Why did natural selection hide our diaphragm from us? Perhaps, as with the heart, our genes don’t trust us to know how to control the diaphragm consciously. Grievously, the body has a vested interest in keeping us from interfering with trauma’s adaptive manifestations. If our environment is seemingly drastic, our genes want us to treat it as such. One of the few times we notice our diaphragms is when we have hiccups. With this in mind, try using the following activity as an alternative route to getting a feel for your diaphragm.
A hiccup is initiated by a reflex arc that produces a spasm of the diaphragm (myoclonic jerk). Hiccupping involves rapid, abrupt diaphragmatic contractions. Of course, this is the opposite of how you want to breathe—i.e., slowly and smoothly. However, hiccupping helps you become acquainted with your diaphragm. Fake a few hiccups, and you will localize your diaphragm in space and sensorium. Another way to sense your diaphragm is to hold your breath for 20 to 40 seconds. You will feel a muscle between your stomach and chest pulsate. This is the diaphragm trying to jumpstart your breathing pattern.
The key to sensing and recruiting the diaphragm is teaching yourself to breathe at a smooth, continuous, and constant rate. This automatically mobilizes the diaphragm because it is what the diaphragm is specialized for and designed to do. Shallow breathing stifles diaphragmatic movement. When the diaphragm is stifled, we use other, less efficient muscles for breathing.

Illustration 3.3: A. Diaphragm, lungs, and respiratory airways; B. Diaphragm shown within and outside the rib cage; C. The phrenic nerves send motor commands to the diaphragm and receive sensory information from it.
Distressed Breathing Utilizes the Thorax and Clavicles
During distressed breathing, the stomach doesn’t move, but the chest does. It involves pivoting the ribs around the joints where they attach to the vertebrae. The thoracic (or intercostal) muscles of the thorax perform this function. The thoracic muscles form the meat in between the bones of barbecued ribs. The external intercostals swing the ribs upward and forward, powering inhalation. The internal intercostals pull the ribs inward and downward, powering exhalation. In a nutshell, diaphragmatic breathing presses the floor of the lungs up and down, whereas thoracic breathing expands the walls of the chest inward and outward. One effect of this difference is that thoracic breathing does not fill the lower portions of the lungs with air, while diaphragmatic breathing does. Thoracic breathing is inherently shallow. It is also less efficient because it requires more work—and more breaths—to transport the same amount of oxygen into your blood.
Clavicular breathing is another form of distressed breathing that involves a shrugging of the clavicles and shoulders. It is even shallower and less efficient than thoracic breathing. It is also called upper thoracic breathing, as it only pulls air into the top third of the lungs. Clavicular breathing is a serious problem, as it can nearly eliminate the function of the diaphragm, leading to even weaker, less effective breaths.
A respiratory physiologist can measure the extent of clavicular and thoracic breathing using electromyography by placing electrodes on the muscles surrounding the clavicles and upper thorax. The electrode readout indicates how active these muscles are and, thus, how defensive the person’s breathing is. You can observe this yourself by paying careful attention to the movement of your shoulders during breathing. If they move up with the in-breath, you are breathing with your clavicles. Clavicular breathing becomes especially pronounced during exercise. In general, you should never breathe with your shoulders. As Chapter 15 will explain, it is preferable to keep the shoulders still and pressed toward the floor.
During ideal diaphragmatic breathing, the thoracic muscles and the diaphragm work together with every breath. The diaphragm should lead the thoracic muscles, setting the pace and making each breath long and smooth. As in the synergy seen between sympathetic and parasympathetic branches of the nervous system, the diaphragm is supposed to work in unison with the thoracic musculature. This synergy falls apart during anxiety when the thoracic musculature and the sympathetic system take over. We have so far encountered two major antagonists in our story about chronic stress. First, we have the overactive sympathetic nervous system. Second, we have overactive thoracic breathing. It should come as no surprise that the two problems collaborate, exacerbating the detrimental effects. The resulting distressed breathing drains our energy, ties knots in our muscles, ages us prematurely, and turns us into nervous wrecks.
The critical link between emotion and stress is the breath. The fear and grief circuitry of the brain activates thoracic breathing and inhibits diaphragmatic breathing. Habitual thoracic or clavicular breathing chronically overstimulates the sympathetic nervous system, keeping heart rate and blood pressure elevated while loading the diaphragm with muscular tension. This causes sympathetic overload. On the other hand, the neural circuitry for self-soothing, mood stabilization, and the calming branch (parasympathetic) of the nervous system is linked to the diaphragm.
There is a simple explanation for this. The diaphragm is structured and situated to contract slowly and steadily to take in just the right amount of air to oxygenate the body at peace. It moves at the optimal rate to procure the proper amount of oxygen needed in a tranquil environment. However, its leisurely pace would be a hindrance to wild animals in a hostile environment.
Thoracic musculature is optimized to produce accelerated breathing during a crisis. Thoracic breathing allows mammals to actively modulate their breaths in response to fluctuations in anticipated danger. In the short run, this would have helped our prehistoric ancestors prepare for the increased oxygen requirements they would need for “fight or flight” maneuvers. Sadly, most of us live in this mode, even though we are no longer protecting our bodies from predators or club-bearing maniacs. The modern world has “tricked” our bodies into thinking that our environment is too stressful to breathe peacefully when the opposite is true.
Distressed Breathing and Social Rank
If you would like to experience pronounced thoracic/clavicular breathing, watch an internet video of a violent street fight and pay careful attention to your breath. The shallow rapidity will become apparent. You could achieve a similar effect just by watching an internet video of an argument between two people. This is because, in primates, social confrontation dysregulates breathing nearly as much as physical violence. When you feel disrespected, cheated, or compelled to explain yourself, you enter a state of respiratory distress. When this happens, people usually act at two extremes, either becoming conflict-avoidant (submissive) or quick to anger.
Respiratory distress is marked by breathing so shallow that it interferes with your speech, causing your voice to falter. You may feel like you are choking and suffocating at the same time. It is usually apparent to those around you, and most people are embarrassed when it happens to them. The truth is that awkward social encounters cause most of us to experience a state of respiratory distress throughout the day.
My experience is that most people have little interest in using breathing exercises to deepen their breath until I explain to them that deep breathing is a dominant trait. Then they become eager. Our respiratory behavior affects our social standing and how we are treated and perceived. People hear changes in the cadence and pitch of your voice that are caused by distressed breathing and use them to make judgments about your level of confidence. Breathing is one of the most common markers of social rank.
Diaphragmatic breathing retraining will make you practically immune to respiratory distress. With enough retraining, people will be able to tell that you have little susceptibility to it. When your breathing shows no signs of distress, people will not want to challenge or provoke you because they realize they will reach respiratory distress before you do. As you develop your capacity for diaphragmatic breathing, you will come to understand that the people around you are constantly fighting wars of attrition to see who will show signs of respiratory distress first.
We also breathe shallowly in a distressed manner to communicate friendliness. Because we don’t want to come across as overbearing or audacious or because we want to make others comfortable, we shorten our breaths and disengage the diaphragm. In other words, we breathe in a distressed manner when we are afraid, when we are mad, and when we are being nice. No wonder it seems inescapable.
Stifling and Neglecting the Diaphragm
Social and environmental stress are not the only causes of distressed breathing. It can also be the result of surgery or injury. After colon surgery, a gastric bypass, a Caesarean procedure, or an appendectomy, for instance, the patient will have an incision wound on their abdomen. It is common for recovering patients to inhibit normal abdominal expansion during breathing to avoid the pain of having their injury disturbed. They learn to actively stifle diaphragmatic movement out of fear of pain or stitches bursting at the incision site. This learned pain avoidance can be long-lasting, causing the patient to neglect the diaphragm and adopt thoracic breathing as a fixed habit. Chronic shallow breathing can result, along with breathlessness and anxiety. It is uncommon for such patients to revert to diaphragmatic use even after the pain from the surgery is gone unless breathing retraining therapy is undertaken.6 You may have never had abdominal surgery, but, to some extent, past trauma and submissive signaling have stifled your diaphragm in a similar way.
Fortunately, we have good models available for how to reinstate diaphragmatic use. The best of these is recovery from a ventilator. In situations where medical patients are having trouble breathing, a machine called an artificial ventilator can be used to move air in and out of their lungs. When a doctor takes a patient off a ventilator, they need to assess the person’s breathing mechanics to ensure the breathing musculature is strong and coordinated enough to support unaided breathing 7 Withdrawal from mechanical ventilation is known as “weaning.”
Think of your thoracic breathing musculature as akin to a ventilator from which you need to wean yourself. Years of stress have caused the thoracic muscles to take control, and your diaphragm has weakened through atrophy caused by disuse. The good news is that the diaphragm can grow stronger quickly. 8
When you first start breathing diaphragmatically, it will be difficult. It will feel as if you have been taken off a ventilator; the muscles you are forcing to breathe for you are not yet up to the job. You will need to wean off thoracic breathing by training the diaphragm. I encourage you to use the exercises in the rest of this chapter to remove the ventilator of thoracic breathing and plunge headfirst into strengthening your diaphragm.
The Four Rules of Diaphragmatic Breathing
In the thick of my anxiety, I could tell that my breathing was highly dysfunctional. I used myself as a model for what not to do and slowly made inferences about how to do the opposite of my acquired tendencies. I read copiously about ventilatory mechanics and experimented with numerous breathing styles. Slowly, after ten years of research, introspection, and trial and error, I developed eight rules of diaphragmatic breathing. This chapter will address the first four, which are:
1) Breathe Deep (high volume): Breathe nearly all the way in by the end of each inhalation and all the way out by the end of each exhalation.
2) Breathe Long (low frequency): Engage in long-interval breathing, breathing in for four to ten seconds and breathing out for six to twelve seconds at a time.
3) Breathe Smooth (continuous flow): Breathe at a steady, slow, nearly constant rate during all breathing.
4) Breathe Assertively (confident): Do not permit social concerns or life stressors to conflict with the first three rules.
 Figure 3.1: A graphical representation of the first three rules of diaphragmatic breathing. The vertical axis designates the depth of inhalation or volume of air in the lungs; the horizontal axis designates time.
Figure 3.1: A graphical representation of the first three rules of diaphragmatic breathing. The vertical axis designates the depth of inhalation or volume of air in the lungs; the horizontal axis designates time.
A helpful way to improve your ability to monitor your breathing is to draw your breathing pattern on paper. Use the examples in Figure 3.1 to work through the exercise below.
After my personal experimentation, I was convinced that adherence to these four rules guaranteed diaphragmatic breathing. I researched these concepts to find support for them in the scientific literature. Further research brought me to the realization that certain clinicians have been using tenets remarkably similar to these for decades. For instance, psychologist Erik Peper developed an excellent system he calls “effortless diaphragmatic breathing,” which consists of a large tidal volume (> 2000ml), slow respiration rate (< 8 breaths per minute), and continuous flow rate.9 Additionally, “Resonant Breathing,” “Coherent Breathing,”10 and the “Conscious Breathing Method”11 are similar breathing methods that I think are scientifically accurate and very helpful.
Related techniques for diaphragmatic breathing retraining have been used by relaxation and biofeedback programs for decades.12 They have also become popular in psychiatry and clinical psychology and are now considered fundamental tools in cognitive behavioral therapy.13 Diaphragmatic breathing, in general, is now touted as an effective, evidence-based stress reduction intervention that is low in cost, easy to use, and can be self-administered with no equipment needed.14 You might be wondering, “How is diaphragmatic breathing defined in medicine?” It’s simple. In the clinical literature, participants are considered as performing diaphragmatic breathing if sensors show that they are breathing longer and deeper (decreasing the respiratory rate while increasing the amplitude of the respiratory waveform).
Diaphragmatic breathing is well known to slow the heart rate and decrease blood pressure. It has been proven to reduce sympathetic arousal, anxiety, panic attacks, and hyperventilation syndrome.15 It is also an effective treatment modality in pain management,16 motion sickness,17 breathlessness,18 and a range of psychiatric and medical disorders.19 For all these reasons, diaphragmatic breathing retraining is used by healthcare providers around the globe.20 Participants in clinical stress reduction programs often report that “the breathing stuff” was the most important thing they learned.
Let’s not forget that diaphragmatic breathing is also an ancient practice. Scientists and clinicians appropriated diaphragmatic breathing methods from India, where they have been used for thousands of years as part of religious and social customs. Diaphragmatic breathing is central to the practice of yoga. Yogis use long, deep inhalations and exhalations. The Buddhist form of meditation called anapanasati (“mindfulness of breathing”) and the Hindu practice of pranayama (“control of breath”) have both explicitly utilized the first two rules outlined above since antiquity. Yoga teachers in every tradition make it clear that the only way to control your mind is to cultivate control of your breath. These sages advocate that we never stop paying attention to it. Yogis who are masters of svarodaya, the yogic science of breathing, claim to be aware of every breath they take.
Diaphragmatic breathing has been around for thousands of years and may just be the most powerful tool in psychiatry, if not medicine as a whole. Why isn’t it more mainstream? How did I finish a formal education in psychology and brain science without being introduced to it? I don’t know for sure, but I think this is partly because it has never been taught correctly. Most existing breathing practices don’t offer a systematic regimen to permanently increase the depth and duration of breathing. Consequently, they don’t provide enough of a benefit to make a substantial difference for most people and, thus, are only used for extreme cases of anxiety. I believe the unique program outlined in this book is so powerful that it can provide substantial benefits for any user. Hopefully, by the end of this chapter, you will agree. Let us continue by looking more closely at each of the four rules
Depth of Breath: Increase Your Tidal Range
The average adult human has a total lung capacity of five to six liters of air, but only a small part of this capacity is used during normal breathing. Nervous breathing will often involve inhalations of less than half a liter. We rarely breathe fully, and most of our breaths are confined to a narrow range. This range is called “tidal volume.” When you increase your tidal volume, which is done by deliberately breathing all the way in and out, you increase your likelihood of accomplishing the other two criteria of longer interval and constant rate.
There is more than one way to deepen your in-breaths, but the exercise below is one of the most straightforward and reliable. It’s based on the work of Joseph Pilates, who saw forced exhalation as the key to full inhalation. He advised his students to squeeze out their lungs as if they were tightly wringing a wet towel. Doing so improves the strength of your breathing musculature quite rapidly. Take advantage of this to increase your tidal range.
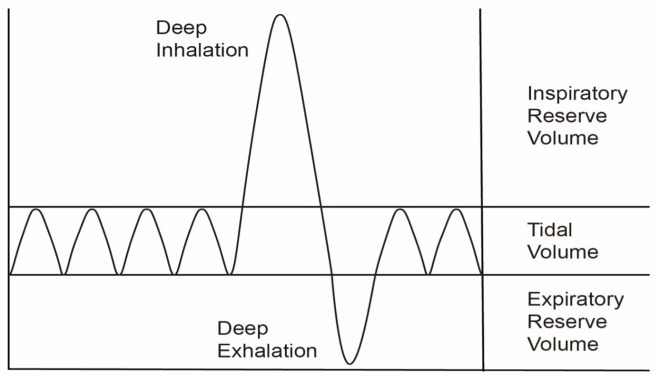 Figure 3.2: This graph shows a sine wave that indicates normal tidal volume. The increase on the fifth breath depicts a deep inhalation that extends the tidal range into the inspiratory reserve. This is followed by a deep exhalation extending the tidal range into the expiratory reserve. Regularly extending the tidal range in this way during breathing training will permanently broaden your default tidal volume and increase the involvement of the diaphragm.
Figure 3.2: This graph shows a sine wave that indicates normal tidal volume. The increase on the fifth breath depicts a deep inhalation that extends the tidal range into the inspiratory reserve. This is followed by a deep exhalation extending the tidal range into the expiratory reserve. Regularly extending the tidal range in this way during breathing training will permanently broaden your default tidal volume and increase the involvement of the diaphragm.
Using an inspirometer while practicing Exercise 3.1 can be very helpful. An inspirometer, which you can purchase online for about ten dollars, is an instrument that allows you to keep track of exactly how much air you can breathe in (vital capacity). Using one consistently can be helpful to track your progress. You might consider monitoring your lung capacity for several weeks with an inspirometer, recording the results and watching your tidal range expand.
At first, it can feel uncomfortable when you breathe all the way in. You might cough. It might feel like your lungs are going to pop. It did for me. Within two months of performing Exercises 3.1 and 3.2, this all changed. There was nothing uncomfortable about being at either the top or bottom of my capacity, and it no longer made me cough. Before the training, it took me six seconds to inhale completely and about ten seconds to exhale completely. After training, it took me only one second to inhale completely and only five seconds to exhale completely. What is more, the maximum I could breathe in, as indicated by the inspirometer, went from 4,000 to 5,000 milliliters.

Illustration 3.4: A. Inspirometer or incentive spirometer; B. Patient on a medical respirator; C. Two chest views from the side depict a narrow diaphragmatic range versus a wide range.
The next activity will help you develop comfort while breathing outside of your normal tidal range. Focus on the uncomfortable sensations that arise. Try to reinterpret them as pleasurable. I try to associate the sensation of taking a full breath with satisfaction, satiety, and fulfillment as if each full breath offers relief and rejuvenating sustenance.
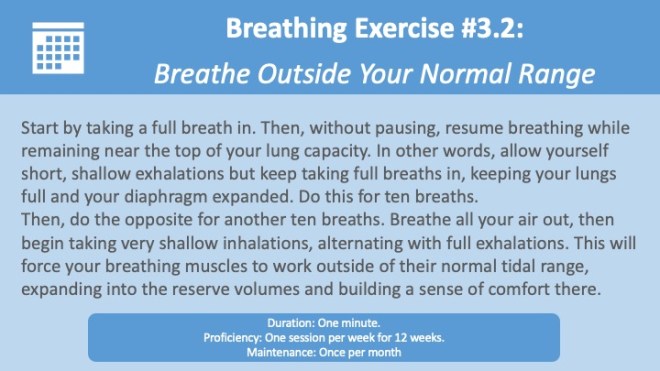
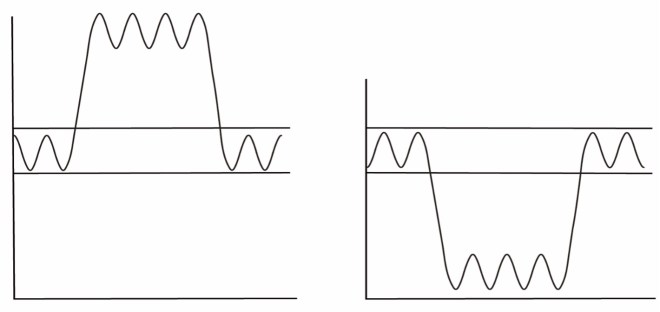
Figure 3.3: A. A graphical depiction of breathing above the normal tidal range for Breathing Exercise 2 above; B. A graph of breathing below the normal tidal range.
Length of Breath: Paced Breathing
The typical adult breathing pattern is marked by shallow thoracic breathing at a rate of 12 to 20 breaths per minute. Many people with anxiety average from 18 to 22, which means each inhalation and exhalation last only one and a half seconds. A breathing therapy technique called “paced breathing” will help you slow this down to a calmer and more grounded five to eight breaths per minute.
The goal of paced breathing is to extend your default habitual breathing rate. Imagine that you customarily breathe at a rate of twenty breaths per minute. If you practice paced breathing at a rate of five breaths per minute for several weeks, the exercise will gradually decrease your default rate from twenty down toward five. The more you practice, the closer your habitual breathing rate will come to the target rate.

Figure 3.4: This graph displays a breathing rate of twenty breaths per minute during the first thirty seconds, then ten breaths per minute during the next thirty seconds, then six breaths per minute, then only two.
The sympathetic nervous system (fight or flight) exhibits reduced activity when a person takes fewer breaths per minute.21 The correlation is direct and immediate. Increasing the number of breaths per minute causes sympathetic nervous system activity to spike, whereas decreasing this number causes it to plummet within one minute.22 If you maintain a rate of five breaths per minute, heart rate and blood pressure drop, nervous sweating declines, and subjective discomfort in response to threat declines significantly.23 There is no easier, faster way to reduce sympathetic activation and the stress it causes. I believe that the most effective intervention for life stress is paced breathing and that it should be used outside of the clinic—by everyone—on a daily basis.
I recommend using a breath metronome (sometimes called a breathing pacemaker) to aid you in pacing your breath. You can download one in the form of a mobile app for your phone or tablet. They generally cost between $1 and $5. All Apple watch users are prompted by the watch to use paced breathing daily. They are guided for one minute to take four breaths (around six-second inhalations and eight-second exhalations). This is a step in the right direction, but to retrain your breathing, it is necessary to spend several minutes per day consciously engaged in paced breathing.
I developed a free app that you can use, called Program Peace: Paced Breathing. It is available for Android and Apple’s iOS. The app gives both audible and visual cues to help you time your breathing. It displays a cylinder that fills and empties in time with your target inhalation and exhalation rate. Alternatively, I offer free downloadable audio MP3 files with paced breathing cues on the Program Peace website. As another option, you can use the breath metronome videos on the Program Peace YouTube channel. My second favorite commercial app is called Breathe 2 Relax. It was developed by the U.S. Department of Defense for veterans and individuals with post-traumatic stress disorder (PTSD). Please take a minute to procure a breath metronome now.
Recommended Breath Metronomes:
- Smartphone and tablet applications: Program Peace: Paced Breathing, Breathe2Relax, Breath Lesson, Breath Pacer, iBreathe, Breathwrk, Breathe Well, Breath Counter, Pranayama, BioBreathing, Calming Breath, Deep Breath, Essence, Tactical Breather.
- Audio MP3 tracks: programpeace.com
- Videos: The Program Peace channel on Youtube
It is very difficult to maintain paced breathing without using an external aid such as a breath metronome. In clinical studies of paced breathing, most participants quickly return to baseline in the absence of an external pacing signal24 You could use a clock or watch, or you could count the seconds in your head, but this quickly gets tiresome and can be extremely difficult to maintain, as it relies on unwavering focus. Unaided, most of us are unlikely to stick with paced breathing for more than a few seconds at a time. By contrast, using a breath metronome frees up your mind to attend to other things. You can do almost any activity with your breath metronome playing in the background. Having one—and familiarizing yourself with its use—is essential because the rest of this book’s exercises will require that you use paced breathing.
Unaided, most of us are unlikely to stick with paced breathing for more than a few seconds at a time. By contrast, using a breath metronome frees up your mind to attend to other things. You can do almost any activity with your breath metronome playing in the background. Having one—and familiarizing yourself with its use—is essential because the rest of this book’s exercises will require that you use paced breathing.

Figure 3.5: The Program Peace Paced Breathing app is free on both Apple and Android devices. It contains a breathing bar on the left side of the screen that rises on the inhalation and lowers on the exhalation.
The next step is to find a reduced “target” breathing rate that will help you slow and deepen your breath without overreaching. Try the rates in the table below for thirty seconds each until you find one that feels challenging but comfortable. For many people, the best starting point is four seconds in and six seconds out, for a total of six complete breaths per minute. This is an extremely healthy way to breathe. I want to encourage you to work up from here toward an ultimate goal of five breaths per minute, which is recommended by many experts.25 It’s fine if you want to stay higher or go lower. This standard of five breaths per minute varies slightly depending on size and age. For adults over six feet tall, the ideal rate is three to four breaths per minute, whereas for children under the age of ten it is between six and nine. Any extension of your breathing interval will be beneficial. Your goal should be to train yourself to breathe at your target rate without any sense of effort or air hunger. Be patient; this will take time. The practice should feel sustainable and good.
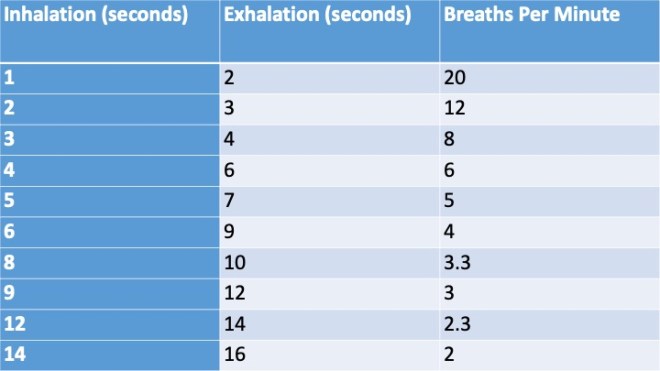
Table 3.1: List of Target Breathing Rates
Notice that in each row in the table above, the exhalation is longer than the inhalation. This is because when you breathe out longer than you breathe in, you activate the vagus nerve, the parasympathetic system, and the body’s relaxation response.26 The longer you can extend your exhalations, the more your autonomic nervous system will be pacified, and the more your heart will decelerate. To augment this calming effect, try to consciously relax during the exhalations. Think of every breath out as a long sigh of relief and the acceptance of a moment of peace. When you’re ready to start, explore your ideal breathing pace by working through the activity below.
When you’re ready to start, explore your ideal breathing pace by working through the activity below.

Try working with the metronome for five minutes before a meeting or a date, and you will be amazed by your level of composure. Practice paced breathing for ten minutes in advance of an interview to give yourself a distinct advantage. At a party, excuse yourself for a few minutes. When you return, you will find your social equilibrium restored. It can help you relax your muscles after a workout, steady yourself after a stressful encounter, prepare for the day, or get to sleep.
Over the next few weeks, find opportunities to include the breath metronome in your daily routines. I often use it in the morning when I wake up, before I go to bed, while reading, while watching TV, while working at my desk, and during my commute. I don’t use the mobile app when driving because pressing buttons on the phone can be distracting and dangerous. Instead, in the car, I listen to the breath metronome mp3s.
Whenever you are doing monotonous busywork or your attention is otherwise free to roam, you can be breathing with a metronome. Watching a movie is a chance for two hours of calming, grounding practice. It can enhance the experience, too—we usually breathe thoracically when we watch film and television because of the suspense and tension that it creates, but paced breathing will de-traumatize your psychological orientation toward even the most intense scenes. Put the metronome on silent and simply hold it in your lap or place it next to the TV, computer monitor, or tablet so that you can use it passively while you attend to other content.
Use it with headphones while walking, gardening, or in the gym. Let your use of it adapt to your routines. Regular use of a breath metronome will help you reestablish optimal breathing, and with it, an optimal life. I think that breath metronomes should be found in every classroom, in every workplace, in every therapist’s office, in every yoga and Pilates studio, in every ambulance, and beside every hospital bed.

Illustration 3.5: A. Mobile phone with breath metronome application for paced breathing; B. Set your phone next to your television so that you can be cued to perform paced breathing while watching your favorite show; C. Grandfather clock with pendulum.
When you start, staying with the metronome can be tricky. If you have not yet filled or emptied the lungs before the metronome switches, go ahead and finish the breath that you are currently on. Quickly inhale or exhale the rest of the air before catching up with the metronome on the next breath. You may feel that you are getting too much air (hyperventilating) or not enough (hypoventilating). This is normal and will pass, but, if it bothers you, just choose a rate that is closer to your default. Work gradually toward a lower rate.
To Avoid Getting Too Much or Too Little Air
- If you are getting too much air or feel dizzy during work with the metronome, simply breathe more slowly. You should be breathing at the same pace but inhaling less powerfully, filling the lungs a little less completely.
- If you are getting too little air or feel faint, do just the opposite and increase the force of your in-breaths. Ensure that you breathe all the way in and all the way out. Sometimes, the metronome will be going too slowly, and you will feel air hunger. If you still feel air hunger, disregard the metronome and take a few deep breaths using whatever timing you need until you are ready to return to your target breathing rate.
Paced breathing involves a learning curve. At first, it takes a fair amount of attention to follow the metronome’s cues and regulate the breath accordingly. After just a couple of hours of cumulative use, you will find that it takes almost no attention at all. This will encourage you to do it more often and allow you to combine it with numerous activities. If you’re having trouble settling on a breathing rate that feels comfortable, use the table below as a rough guide. It lays out estimated breathing rates for what your target pace should be under different conditions and cardiovascular demands
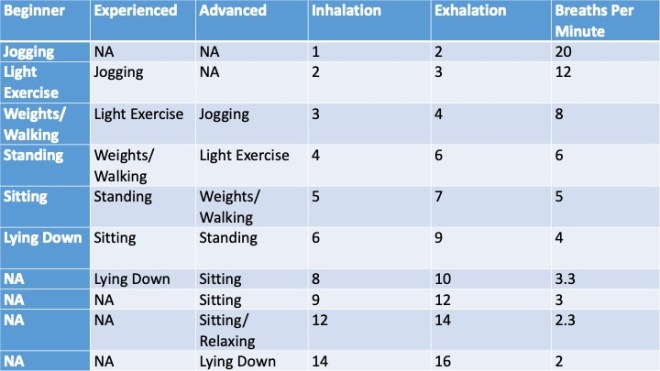
Table 3.2: Comfortable Breathing Rates by Experience and Level of Physical Activity
When Not Using a Breath Metronome:
1) Try to focus on your breathing frequently throughout the day, monitoring it and deciding whether it is too shallow or too fast. If so, consciously deepen your breath.
2) Catch yourself preparing to switch prematurely from breathing in to breathing out (or vice versa) before you have taken a full breath. Instead of switching, prolong the tail end of the breath in which you are currently engaged.
Advanced paced breathing at a rate of fewer than four breaths per minute can be powerfully relaxing. I should point out that it is not a comfortable or realistic default breathing rate, but training at this rate will help improve your default rate and train smooth breathing, which is the topic of the next section.
Smoothness of Breath: Breathing at a Constant Speed
The third element of healthy diaphragmatic breathing is the smoothness of your breath. This is a question of how fluidly you breathe, and it ties together the previous two elements of your practice. Paced breathing and deep breathing can still allow for too much variability on a moment-to-moment basis. This is where the flow rate of each in-breath and out-breath becomes important.
For instance, at the beginning of my practice, about halfway through each five-second inhalation, the speed of my breath would drop, leaving the second half of the inhalation weaker. After this lapse, I would try to make up for it at the very end of the five seconds by gasping. I was being lazy, holding my breath mid-count to get out of doing the work of strengthening the diaphragm. Instead, we should try to breathe at the same rate throughout each breath to keep the diaphragm engaged. This involves breathing slowly, gently, and steadily.
The biggest barrier to smooth breathing is our tendency to switch from diaphragmatic to thoracic inhalation when you near the top of your tidal range. Every inhalation begins with the diaphragm, but once using the diaphragm outside of its default range, we transition to a swift thoracic inhalation to draw in that last bit of air. Resist this instinct. Instead, try to get to the top of your inspiratory reserve using only the diaphragm by breathing slowly and gradually. Do the exercise below to practice using your diaphragm throughout the entire inhalation.

You experienced the impulse to switch to a rapid thoracic inhalation in the exercise above because your diaphragm is not accustomed to providing steady suction for a breath outside its normal tidal range. I think of this weakness as a diaphragmatic speedbump at the end of the diaphragm’s habitual path. Forcing smooth inhalations steadily past this range will rehabilitate the muscular knot in your diaphragm responsible for this speedbump. It will also accustom your nervous system to utilizing the diaphragm more fully. Breaking down this restriction that limits your diaphragm’s range of motion is unique to the Program Peace system yet integral to diaphragmatic retraining.

Figure 3.5: A. Each of the three graphs starts with four shallow breaths for comparison. In the first graph, the fifth inhalation is deep and long. However, the inhalation does not occur at a constant rate (the slope of the line varies). As you can see, it plateaus three times and ends with a gasp. This person is gasping and breath holding because they are uncomfortable breathing above their normal diaphragmatic range; B. The fifth inhalation in the second diagram is also very deep. However, it is short in duration, so it is basically a thoracic gasp (the line’s slope is very high); C. The fifth inhalation in the third diagram shows the optimal breathing pattern of a long, deep inhalation at a steady rate (with a constant slope).
As you practice, keep your flow rate steady by imagining yourself smelling a rose, inhaling very slowly as you savor its fragrance. Or imagine that you are curled up with a small pet. Make your breathing as smooth and calm as possible to soothe it gently to sleep. Realize that hasty, quivering, jerky breaths would likely rouse and frighten it. It is interesting to note that when a cat purrs, its breathing is slow, even, and powered by the diaphragm.27 Above, I recommended that you invest ten dollars in an inspirometer to monitor the depth of your breathing. If you do so, purchase one with a flow rate indicator. This will provide real-time feedback on how steady and smooth your breathing is.
Another option is to buy yourself a stethoscope to listen to your breathing. You can find these for around $15 online. When you put the “bell” of the stethoscope up to your mouth, you can hear tiny distortions and discontinuities in the breath—desperate little gasps. These gasps are more noticeable when you are self-doubting and are sometimes described as “fluttering” or “catches” in the breath. It sounds a bit like the voice when it “cracks.” While listening to these distortions in my breath, it became clear to me that breathing, especially breathing deeply, is a struggle. It doesn’t have to be.
The more slowly and fully you breathe outside of your tidal range, the more you can hear and feel these points of weakness in the breath. The technical term for them is apneic disturbances, and they usually last for tiny fractions of a second. They are such a basic feature of most people’s breathing that they seem natural and normal, but they are suboptimal without a doubt. These disturbances are caused by weakness in the diaphragm and correspond to absences in its range of motion. They are linked to the startle response and keep you feeling on edge. As the next activity shows, you do not need a stethoscope to hear these.

Illustration 3.6: Person cupping their hands from mouth to ear to amplify the sound of the breath; B. Depiction of a discontinuous, rough breath compared to a continuous, smooth breath.
Buddhist and Hindu practices emphasize breathing through the nose and down the back of the throat. Many meditators concentrate on the “ha” or “so” sound this produces. Creating an even sound throughout each breath will ensure that the breath is being taken in at an even rate. To do this, focus on maintaining the same sound from the beginning of each inhalation/exhalation to the end. You know you are breathing diaphragmatically if the sound of your breath is not changing. Other ways to make sounds that you can monitor for constancy include breathing as if you are fogging up glass, making a hissing sound with your tongue, a “haaaa” sound with your voice, a buzzing sound with your throat, or a glottal sound with your vocal folds. Many meditators use mantras to accomplish this. Using a stethoscope, cupping your hands, or making a sound of some kind all accomplish the same thing. So, perform Exercise 3.4 using any of these methods.
I was concerned the first time I heard my breath amplified by a stethoscope because I immediately recognized that these irregular pauses and gasps were unhealthy. The irregular pauses are magnified by adversity and are responsible for the sensation of respiratory distress. Breathing is strained whenever a single inhalation pauses, slows, or speeds up. When someone is stressed, you can often hear them straining for more breath, as multiple rapid gasps or shudders will punctuate the inhalation. The gasps occur when one is continuing to inhale despite their body’s inclination to “switch” to exhalation. The weakness in the breath tells us to stop taking a full inhalation and go back to exhaling prematurely. This is the same mechanism that causes us to breathe shallowly, and that creates the diaphragmatic speedbump. This phenomenon of fighting against oneself for breath is sometimes called paradoxical breathing.
We are constantly modulating the rate of each breath from second to second, depending on our level of air hunger and transient stress. We may alter the rate of a single breath many times. This is not ideal. Tell yourself that you will stick with the same rate for the entirety of each breath. If you need to change the rate because you need more air, change at the beginning of the next inhalation or exhalation, but not during an actual breath. One helpful way to assist you in this is through breathing exclusively through the nose, which we will discuss in Chapter 11.
Imagine that your breath is an accordion that you have spent your life thrusting and thrashing in a distraught, feverish way. Imagine now playing the accordion by moving your hands very slowly and continuously stretching the accordion out to its full length and then gently pressing it closed, over and over.
People who perform intricate manual work, or marksmen who shoot targets, find that holding the breath helps steady the hands. Once you reprogram your breath to be continuous and smooth, breath-holding is no longer necessary to keep you from shaking. As you paint an eyebrow on that tiny face on your canvass or take aim at a distant target, you will find yourself smoothing out your breath rather than holding it.
Distressed breathing progresses like an automobile that is alternating between stalling and redlining. You want your breathing to be like a reliable car, engine purring, on a smoothly paved freeway, with the cruise control on.
Breathe Assertively
So far, we have covered methods for breathing smoothly, deeply, and at longer intervals. The fourth rule is to breathe assertively. We usually breathe as if we don’t have any faith in our breath. A thoracic breather knows that a negative thought could interrupt the breath at any time by prematurely turning an exhalation into an inhalation or vice versa. This causes them to breathe not only shallowly but cautiously and hesitantly as if they are tiptoeing. It also keeps them from breathing efficiently because they are not taking advantage of inertia. If a breath proceeds steadily, it can capture its own momentum, resulting in reduced effort. During hesitant, unsteady breath, the breathing musculature is constantly building and then losing momentum.
Model your breathing on the motion of a pendulum or some other uninterrupted, inevitable oscillating process. Something that moves with certainty. Each stroke of a pendulum fully captures its momentum until gravity reverses the swing. Any pendulum would be useless if it slowed or stopped midway. Picture your diaphragm stroking up and down in a slow but unfaltering, unagitated way. Breathe out with certain knowledge that you are not going to switch prematurely to a gasp. Commit to each breath steadfastly.
To feel comfortable breathing with confidence, you will need to be willing to let the people around you hear your breath. You must not be afraid of being heard or noticed. Instead, be proud of how your breath does not waver, falter, or hesitate. Don’t think that people will hear it and be offended. Breathe decisively and audibly if necessary, for all to hear. Breathing assertively is the demonstration of true aplomb. Start by using your imagination.
Many people who are widely admired and described as charismatic are merely assertive breathers. The self-taught dog behaviorist, Cesar Millan, is one such person. He is widely known for his Dog Whisperer television series, in which he works with aggressive and abused dogs. In 2009, The New York Times attributed his success to his sense of equanimity, describing this as, “a sort of uber-balanced mien.”28 Millan calls it “calm-assertive energy” and says that he approaches dogs as a pack leader.29
There is good reason to believe that Millan’s effect on dogs derives from his breathing. Throughout the episodes of his TV series, his breathing remains calm, constant, and resolute despite repeated problematic encounters with both the dogs and their owners. Cesar Millan and people like him have an autonomous breathing pattern that is not susceptible to being stopped short by the behavior or misbehavior of others. Dogs are in tune with how the status hierarchy is conveyed through breathing. I think the dogs know there is nothing they can do to disturb his breathing, so they listen to and respect him. Millan’s techniques work as well on abused and subordinated dogs as on aggressive and intractable ones.
Respiratory rates, and fluctuations in them, constitute a language that all mammals speak. Try sitting near your cat or dog, breathing calmly, and then suddenly switch to short, quick, loud breaths. The animal will become concerned, appear nervous, and adopt your breathing pattern. If, instead, you breathe slowly and deeply, they are likely to relax, yawn, and start stretching. If you breathe slowly and deeply while training or correcting them, they will heed you.
Health practitioners often need to assess their patients’ respiratory rate, the number of breaths (inhalation-exhalation cycles) taken within 60 seconds. The method a doctor or clinician uses to measure the respiratory rate of a child, an animal, or an adult can affect the measurement. Simply handling an animal will increase its respiratory rate, giving a false reading, unless the animal is handled very gently, in which case its respiratory rate may fall. Using a cold stethoscope to measure respiratory rate in a child will increase their respiratory rate, whereas other less “obtrusive” methods (like counting the number of times the chest rises) may not.
Clinical texts refer to the “invasiveness” of different methodological procedures for assessing respiration. A doctor that acts either domineering or too accommodating can raise it. Different aspects of our environment are constantly “invading” our respiratory dynamics. Don’t allow your breathing rate or depth to be dictated by banal occurrences in your environment. Confidence starts with assertive, uninterruptable breathing.
The Connection Between the Breath and the Mind
Feelings of pain and frustration are compounded by shallow breathing. Pride, vanity, and guilt are also ramped up by distressed breathing, and I will focus on these relationships in later chapters. Shortness of breath makes us feel like we are suffocating. In such a state, we can’t help but think negative thoughts. Once you have internalized the four rules and are breathing deeply, smoothly, and at long intervals, it will become clear to you that the mental bondage chaining us to our ego and the social hierarchy is severed when breathing diaphragmatically.
The discomfort from shallow breathing magnifies many addictive behaviors by making us feel desperation. Our breathing becomes shallower when we are hungry, thereby strengthening our cravings for food. People use the phrase “I’m starving” when they notice that their hunger is affecting their breathing. Similarly, many people turn to cigarettes, alcohol, and anger when they feel their breathing affected by unfavorable life circumstances. When people use drugs to change their emotional state, they are really changing the state of their breathing.
One can transform disordered breathing into quasi-healthy breathing in minutes using barbiturates, sedatives, or opiates. However, that effect is short-lived, and the inevitable withdrawal symptoms actually accentuate disordered breathing. By contrast, metronome-aided paced breathing kicks in faster than drugs or alcohol and makes you a stronger person rather than a weaker one. Over time, expect paced breathing to vastly increase your distress tolerance and your capacity for emotional regulation.
After I started practicing paced breathing, I experienced a process of self-re-creation. At the end of this process, I had a new aura, a new persona, and a new relationship with others. The change within me elicited a different set of reactions from the people I encountered. Strangers initiated pleasant conversations with me. Individuals in crowded, public spaces were polite and, at times, even kind. I was more easily accepted in groups and committees. I found that children and animals approached me without hesitation. However, it made some adult males uncomfortable. People who are competitive with you may assume at first glance that your undaunted breathing pattern is a façade. But, even after a brief interaction, they will realize you are not faking it.
You can’t feign the poise made possible by diaphragmatic retraining. Distressed breathing, on the other hand, is a signal to predators that you are in panic mode. When someone “smells fear,” they are actually sensing distressed breathing. It tempts bullies to close in for the kill and tends to intensify arguments into fights. Diaphragmatic breathing does the opposite by broadcasting assertive, noncombative calm. Diaphragmatic breathing safeguards you from violence, whereas thoracic breathing invites it.
Many people only breathe easy in social situations in which they are with someone they feel they can patronize and talk down to. We should be breathing easy no matter who we are with. What people think about you, how they are judging you, and their current level of displeasure should not be a factor in the equation that determines your ease of breathing. I used to try to breathe more shallowly than everyone else around me to be polite. This quickly becomes dangerous to your health. You may not feel comfortable with how secure you appear to others when you breathe slowly and diaphragmatically. You may feel there is incongruence between it and your level of attractiveness, strength, or socioeconomic status. I’m writing to promulgate the idea that there is never incongruity among these things.
A part of us is afraid that breathing calmly around others is the ultimate insult. We are afraid that the other person will become angry if s/he sees us breathing too deeply. We breathe the most shallowly around the most dominant people in our lives. This is partly because when we breathe deeply, our emotional reactivity decreases and our facial response time is delayed. Our faces become calmer and may appear less attentive. You might feel that this makes you look distant or disconnected.
You will notice that you breathe at long intervals during a conversation, that your face goes blank and non-expressive. We need to get over the fear that someone will see us and think that we look too calm. As Chapter 7 will discuss, there should be no such thing as looking too calm. The best way to train this is to try to retain diaphragmatic breathing during all social encounters. It will become sincere with practice. Don’t let outside influences or internal fears about them perturb your optimal breathing pattern.
Breathe Diaphragmatically in Public
Diaphragmatic breathing in public is truly transformative. When you first try it, it will reveal your tendencies for agoraphobia and social anxiety. Within a few minutes, you will start to overcome them. Here’s what to do. Take your breathing app with you to a restaurant, coffee shop, café, picnic table, or bench in the park. Then, using headphones, listen to your breath metronome’s auditory breathing cues to practice paced breathing. You will gradually feel yourself letting go of social uneasiness. As this new attitude becomes your default, you will lose your apprehension about potentially negative social outcomes, making your outward appearance more assertive and less defensive. Other people will see in your face that you are not afraid. You will start to appraise the vast majority of people as harmless. Instead of being a potential assailant or judgmental critic, each person will become just another face.

Breathe Diaphragmatically While Speaking
Once you’ve become familiar with breathing diaphragmatically in public, try it in conversation. This is more difficult. Many of us become short of breath during social encounters, especially when public speaking. I used to fully inhibit my diaphragm as soon as I began speaking. At first, I tried workarounds, like taking intermittent breaks from conversation to regain my composure. But that was socially disruptive. What you want is to learn to breathe deeply and diaphragmatically while speaking. This isn’t easy because you must formulate what you want to say and simultaneously focus on monitoring your breath.
The best way to start is to read aloud while breathing diaphragmatically. It will likely be uncomfortable at first because we all normally speak within a very narrow tidal range. The trick to calming your speech is to prolong your speaking time and ensure that anxious gasps do not punctuate it. The following exercise will guide you through the process (note that it does not use a breath metronome).
Find your limit—how long you can read without inhaling—and then repeat that level of performance over and over. To determine where that limit is, try reading the remainder of this paragraph without breathing in. Continue until you cannot possibly speak another word. There should be a few seconds at the end where your voice changes appreciably and it becomes very uncomfortable to speak. Your voice will begin to waver and lurch. You will sound like someone in extreme respiratory distress, and it may even start to feel like you just got punched in the chest. If you work on Exercise 3.7 in this manner for only a few minutes every day, you will, in short order, alleviate this impediment and any related discomfort.
Breathe Diaphragmatically During Exercise
Another effective way to strengthen your diaphragm is to pair diaphragmatic breathing with a cardiovascular workout. Try taking a short jog, focusing on the sensations you feel when alternating between inhalations and exhalations. You are likely alternating far too quickly. Try blowing nearly all the way out and breathing nearly all the way in with each breath. This can feel uncomfortable but is extremely healthful.
Ironically, many people breathe shallowly while exercising because they are concerned they will not get enough air if they breathe too deeply. The sensation of elevated heart rate makes you want to take tiny breaths. Ignore the panic signals from your heart and ensure that you breathe in and out near full capacity. As long as you are breathing heavily, you are getting plenty of oxygen. When you persist in an exhalation, even when you feel your heart beating hard in your chest, you are restructuring your unhealthy breathing patterns and breaking through the trauma that underlies them. Don’t bother using your breathing metronome during cardio, just make sure you are taking full breaths. Use the next exercise to get you going.
Breathe Diaphragmatically While Eating
There’s one other daily activity that deserves specific attention. It is surprisingly difficult to follow a breath metronome while eating a meal. Attempting it makes us aware of just how entangled our appetitive drives are with distressed breathing. The first time I tried it, I realized that distressed breathing had created a starving, ravenous creature inside of me. The activity below offers a puzzlingly difficult challenge that should pique your interest in the benefits of diaphragmatic breathing. The last two activities do not require the use of a breath metronome, but this activity, like most of the activities in this program, is greatly improved by using one.
Generalizing Diaphragmatic Breathing
For many people, distressed breathing is pervasive and affects every aspect of daily life. This book aims to help you develop just the opposite: an ingrained habit for deep, diaphragmatic breathing that you practice every waking moment. As Chapter 1 explained, this new habit will desensitize your stress system by pairing experiences that are normally stressful (and linked to thoracic breathing) with diaphragmatic breathing instead.
I was partially inspired to create a system based on this concept by my experiences in the yoga studio. Hatha yoga revolves around yoking various stretches and poses with calm breathing. Since developing the present program, I have found that this concept is not even new in the clinical arena. It is a little-known technique called “generalization of diaphragmatic breathing.”
Some therapists use diaphragmatic generalization to help clients associate peaceful breathing with distressing thoughts and other activities such as standing, sitting, and walking. Forming those associations ensures that proper breathing predominates in most life situations.30 Yoking relaxed breathing to various activities in this way can be considered a form of systematic desensitization.
Systematic desensitization is a psychological method used to help people overcome phobias and anxieties. It is a popular form of exposure therapy that uses counter-conditioning (a Pavlovian process) developed by South African psychiatrist Joseph Wolpe. The idea is simple:
If the source of the person’s anxiety is discovered (i.e., spiders), the person is trained in relaxation techniques (i.e., reappraisal, breathing, and muscle relaxation exercises) and then guided to use these techniques while they are exposed to increasing levels of fear-inducing stimuli. They might progress from talking about spiders to looking at pictures of spiders, then to videos of spiders, and finally to holding real spiders. Their fear of spiders is thus brought to extinction by gradual exposure. This cognitive-behavioral therapy technique is considered one of the most effective in clinical psychology today.31 It is used to help people become comfortable with all kinds of stressors, including things like elevators, dogs, knives, and public speaking.
As the last three exercises have illustrated, you can apply the same principle to the simplest of behaviors. If you can maintain diaphragmatic breathing while you gradually and systematically perform actions that would normally increase your breathing rate, you can habituate to these stressors and reprogram the way your breathing system relates to them. Taking this a step further, you can even desensitize yourself to your attempts at assuming dominant or optimal postures that would normally cause you to breathe shallowly.
The rest of this book’s exercises are intended to be performed with paced diaphragmatic breathing, guided by a breath metronome. This is done to make every nonsubmissive posture a safe and fun “place to be.” Having spent more than ten years pairing hundreds of different activities with diaphragmatic breathing, I am sharing the ones that benefited my clients and me the most. Below is the fundamental diaphragmatic breathing exercise that I would like you to combine with every other exercise and activity in the remainder of this book (please note that Exercise 1.1 from Chapter 1 can be used as an alternative to breathing with a metronome).
Here’s a way to quickly and easily get a sense of just how powerful generalized diaphragmatic breathing can be. I am going to ask you to do a deep backbend without paced breathing, and then again with it. Lie down on your stomach on a carpet, bed, or soft surface. Then, use your arms to lift your torso off the ground while your legs and hips lie flat, performing a gentle “upward dog” pose. Notice how shallow and irregular your breathing becomes when you do a backbend? Lie back down and imagine what it would take for you to improve your upward dog. Lots of time and effort, right? Years of yoga training? Not quite.
Spend five minutes practicing the paced breathing method in Exercise 3.10 above. Now, try the upward dog again. The position should be easier to hold and less stressful to perform. Your back should feel supported and safe, rather than exposed and vulnerable, and you should have a sense that you are stretching and strengthening your lower back rather than straining it. The reason this works so well is that diaphragmatic breathing affects muscles directly. Chapter 5 will address how distressed breathing makes muscles throughout your body close down with tension, while diaphragmatic breathing makes them receptive to being toned.
Every time you repeat a breathing exercise, you make innumerable cellular and molecular improvements to the function of your muscular, nervous, and respiratory systems. These beneficial alterations accumulate. As a bonus, all the mental work involved in learning to incorporate the diaphragm into your breathing is saved to procedural memory—in other words, routinized—which makes diaphragmatic breathing easier in the future.
Conclusion
After six months of paced breathing, I decided to try belly breathing again. This is the activity in which one places a hand on the chest and another on the abdomen to check for natural movement of the stomach with breathing (outlined in Activity 3.2 in this chapter). Before I started, there was nothing I could do to use my breath to raise my abdomen. Only half a year later, my abdomen rose and fell on its own with every breath. To get your diaphragm back in the groove, work toward the following goals:
- Belly breathing: once you’ve been pace breathing for a few months, every breath should move your belly.
- Aim to iron out all the apneic disturbances in your breath by breathing right through them, slowly and smoothly.
- You want deep inhalations and exhalations that reach the very end of their range to feel comfortable.
- Work toward increasing the target breathing rate you picked for yourself earlier in this chapter.
Your goal should be to progress to the point where you are training somewhere in the vicinity of five breaths per minute (5×7). Once you have trained here comfortably for around a dozen hours, you will be belly breathing. Spending time practicing at a much lower rate, such as 10×12, is slower than optimal for everyday breathing but amounts to a form of cross-training that will help strengthen you overall.
To accomplish these goals as quickly and efficiently as possible, I recommend spending at least 20 minutes each day practicing paced breathing with a breath metronome. That may sound like a lot, but it is easy. You can do it while you watch TV. In the coming chapters, we will talk a lot more about the breath and introduce four more tenets of optimal breathing. In Chapter 11, we will return to the material from this chapter and view it from the perspective of hyperventilation and nasal breathing. In the next chapter, though, let’s put what you have learned about paced breathing to work and pair it with exercises intended to rehabilitate the windows to the soul: the eyes.
Chapter Three: Bullet Points
- The brain’s fear and grief circuits are tied to distressed breathing. They inhibit the diaphragm, causing breathing to become rapid and shallow.
- The more traumatized a mammal is, the less its diaphragm moves with each breath. The animal instead recruits other muscles to power breathing and the diaphragm atrophies.
- Disuse due to stress reduces the diaphragm’s range of motion and causes it to become stiff.
- Most people breathe in a narrow diaphragmatic range. This range narrows further as stress increases. You want to expand your diaphragm’s range of motion by breathing more deeply.
- To engage the diaphragm fully, follow these four rules: (1) breathe deeply, (2) breathe at long intervals, (3) breathe smoothly, and (4) breathe assertively.
- Breathing slowly, deeply, and smoothly forces the diaphragm to contract evenly, increasing diaphragmatic strength, coordination, and range of motion.
- It is common for people with anxiety to have inhalations that merely last one second and exhalations that last only two seconds.
- To rehabilitate our breath, we should practice breathing at least three seconds in and five seconds out (3×5). To make this your default breathing rate, it helps to practice breathing at even longer intervals. Performing paced breathing at 5×7 and working toward 10×12 will accomplish this.
- Weakness in the diaphragm is apparent in the form of tiny gasps or unevenness in the breath, called apneic disturbances, which are associated with the startle response.
- You can iron out apneic disturbances by breathing smoothly at a slow and even rate.
- Breathing assertively involves making sure that social concerns do not interfere with the first three rules. You want to breathe deeply, smoothly, and at long intervals while you are socializing.
- Using a breath metronome daily is essential to developing a strong diaphragmatic breathing habit because it will allow you to train yourself to follow the four rules while you focus on other tasks and activities.
- Monitor your breathing carefully during conversations; don’t let it become shallow.
- Your breath should be a tiny but continuous sip of air that never pauses and always proceeds at a steady rate.
![]()
Endnotes
- Meuret, A. E., & Ritz, T. (2010). Hyperventilation in panic disorder and asthma: Empirical evidence and clinical strategies. International Journal Psychophysiology. 78(1), 68–79; Lum, L. C. (1987). Hyperventilation syndromes in medicine and psychiatry: A review. Journal of the Royal Society of Medicine. 80(4), 229–231.
- Ravinder, J., Crawford, M., Barnes, V. A., & Harden, K. (2015). Self-regulation of breathing as a primary treatment for anxiety. Applied Psychophysiological Biofeedback, 40(2), 107–115.
- Hamasaki, H. (2020). Effects of diaphragmatic breathing on health: A narrative review. Medicines (Basel), 7(10), 65.
- Lippincott, W. & Wilkins (2006). Stedman’s medical dictionary (28th ed). Julie K. Stegman.
- Farhi, D. (1996). The breathing book: Good health and vitality through essential breath work. Henry Holt.
- Ford, G. T., Whitelaw, W. A., Rosenal, T. W., Cruse, P. J., & Guenter, C. A. (1983). Diaphragm function after upper abdominal surgery in humans. The American Review of Respiratory Disease, 127(4), 431-6.
- McConville, J. F., & Kress, J. P. (2012). Weaning patients from the ventilator. New England Journal of Medicine, 367(23), 2233-2239.
- Levine, S., Nguyen, T., Taylor, N., Friscia, M. E., Budak, M. T., Rothenberg, P., Zhu, J., Sachdeva, R., Sonnad, S., Kaiser, L. R., Rubinstein, N. A., Powers, S. K., & Shrager, J. B. (2008). Rapid disuse atrophy of diaphragm fibers in mechanically ventilated humans. New England Journal of Medicine, 358(13), 1327–35.
- Peper, E. & Tibbetts, V. (1994). Effortless diaphragmatic breathing. Physical Therapy Products. 6(2), 67–71.
- Elliot, S., & Edmonson, D. (2008) Coherent breathing: The definitive method, theory, and practice. Coherence Press.
- Olsson, A. (2014). The power of your breath. The secret key to reshaping your looks, your body, your health, and your weight. Anders Olsson.
- Gevirtz, R. N., & Schwartz, M. S. (2003). The respiratory system in applied psychophysiology. In M. S. Schwartz & F. Andrasik (Eds.), Biofeedback: A practitioners guide (3rd ed., pp. 212–244). The Guilford Press.
- Hazlett-Stevens, H., & Craske, M. G. (2009). Breathing retraining and diaphragmatic breathing techniques. In W. T. O’Donohue & J. Fisher (Eds.), General principles and empirically supported techniques of cognitive behavior therapy (pp. 166–172. John Wiley & Sons.
- Hopper, S. I., Murray, S. L., Ferrara, L. R., & Singleton, J. K. (2018). Effectiveness of diaphragmatic breathing on physiological and psychological stress in adults: A quantitative systematic review protocol. JBI Database of Systematic Reviews and Implementation Reports, 16(6), 1367–1372.
- Gervitz & Schwartz, 2003, The respiratory system in applied psychophysiology.
- McGeary, C. A., Swanholm, E., Gatchel, R. J. (2014) Pain management. The encyclopedia of clinical psychology. John Wiley & Sons.
- Stromberg, S. E., Russell, M. E., & Carlson, C. R. (2015). Diaphragmatic breathing and its effectiveness for the management of motion sickness. Aerospace Medicine and Human Performance, 86(5), 452–457.
- Borge, C. R., Mengshoel, A. M., Omenaas, E., Moum, T., Ekman, I., Lein, M. P., Mack, U., & Wahl, A. K. (2015). Effects on guided deep breathing on breathlessness and the breathing pattern in chronic obstructive pulmonary disease: A double-blind randomized control study. Patient Education and Counseling, 98(2), 182–190.
- Vranceanu, A., Gordon, J. R., Gorman, M. J., & Safren, S. A. (2016). Behavioral medicine strategies in outpatient psychiatric settings. In T. Petersen, S. Sprich, & S. Wilhelm (Eds.), The Massachusetts General Hospital handbook of cognitive behavioral therapy (pp. 243–257). Springer.
- van der Kolk, B. A., Stone, L., West, J., Rhodes, A., Emerson, D., Suvak, M., & Spinazzola, J. (2014). Yoga as an adjunctive treatment for posttraumatic stress disorder: A randomized controlled trial. Journal of Clinical Psychiatry, 75(6), e599–565.
- Lichstein, K. L. (1988). Clinical relaxation strategies. Wiley-Interscience
- Elliott, S., & Edmonson, E. (2006). The new science of breath: Coherent breathing for autonomic nervous system balance, health, and well-being. Coherence Press.
- Gervitz & Schwartz, 2003, The respiratory system in applied psychophysiology.
- Clark, M. E., & Hirschman, R. (1990). Effects of paced respiration on anxiety reduction in a clinical population. Biofeedback and Self-regulation, 15(3), 273–284.
- Brown, R. P., & Berbarg, P. (2012). The healing power of the breath: Simple techniques to reduce stress and anxiety, enhance concentration, and balance your emotions. Shambhala Publications; Gervitz & Schwartz, 2003, The respiratory system in applied psychophysiology.
- Bae, D., Matthews, J. J. L., Chen, J. J., & Mah, L. (2021). Increased exhalation to inhalation ratio during breathing enhances high-frequency heart rate variability in healthy adults. Psychophysiology, 58(11), e13905.
- Remmers, J. E., & Gautier, H. (1972). Neural and mechanical mechanisms of feline purring. Respiration Physiology, 16(3), 351–361.
- Wallace, A. (2009, October 11). Whispering to Rottweilers, and to C.E.O.’s. The New York Times.
- Millan, C., & Peltier, M. J. (2006). Cesar’s way: The natural, everyday guide to understanding & correcting common dog problems. Random House.
- Peper & Tibbetts, 1994, Effortless diaphragmatic breathing.
- McGlynn, F., Smitherman, T., & Gothard, K. (2004). Comment on the status of systematic desensitization. Behavior Modification, 28(2), 194–205.